Three clients asked me about Ozempic this week alone.
Not from a doctor’s recommendation. From Instagram reels. From a colleague at work who “lost 8 kgs without doing anything.” From a WhatsApp forward about a ₹1,290/month injection that “melts fat.”
Here’s the thing: they’re not entirely wrong. Peptides are real science. Semaglutide has some of the strongest clinical evidence of any weight loss intervention ever studied. And as of March 2026, generic semaglutide is available in India from 40+ manufacturers at a fraction of what Ozempic used to cost.
But the full picture is more complicated than any Instagram reel will show you. This is what I tell every client who asks.
What Are Peptides, Actually?
Peptides are short chains of amino acids — the same building blocks that make up the proteins in your dal and paneer. Your body produces thousands of peptides naturally. They act as signalling molecules: telling your cells what to do, when to grow, when to repair, when to release hormones.
When people say “peptides” in the fitness context, they’re usually talking about one of two categories:
- FDA-approved GLP-1 drugs — semaglutide (Ozempic/Wegovy), tirzepatide (Mounjaro). These have extensive clinical trial data and are prescribed by doctors.
- Research peptides — BPC-157, TB-500, Ipamorelin, CJC-1295, and others. These are promoted by fitness influencers, sold online as “research chemicals,” and have little to no human clinical data.
These two categories could not be more different. Lumping them together — as most social media content does — is dangerous.
The GLP-1 Revolution: What the Science Actually Says
Let’s start with what works. Semaglutide and tirzepatide are the most well-studied weight loss drugs in history.
The numbers from clinical trials:
- Semaglutide (Wegovy): 13.7% average body weight loss over 72 weeks in the STEP-1 trial
- Tirzepatide (Mounjaro): 20.2% average body weight loss over 72 weeks — the most effective weight loss drug ever studied
These aren’t small effects. For a 90 kg person, that’s 12-18 kg lost.
They work by mimicking GLP-1, a hormone your gut naturally releases after eating. GLP-1 tells your brain you’re full, slows stomach emptying, and improves insulin sensitivity. The drugs just amplify this signal.
The India Story: ₹1,290/Month and Counting
On March 20, 2026, Novo Nordisk’s core Indian patent on semaglutide expired. Within days, over 40 Indian generic manufacturers launched their versions.
The price collapse was dramatic:
- Branded Ozempic: dropped to ₹5,660/month (from ₹8,800)
- Generic semaglutide (Natco, Glenmark, Sun Pharma, Dr. Reddy’s, Zydus): starting from ₹1,290/month
That’s a 90% price drop. Semaglutide went from an expensive imported drug to something more affordable than most gym memberships.
This is why everyone is suddenly talking about it. It’s not that the drug is new — it’s that it’s now accessible.
The Part Nobody Talks About: Muscle Loss
Here’s where I start having a real conversation with my clients.
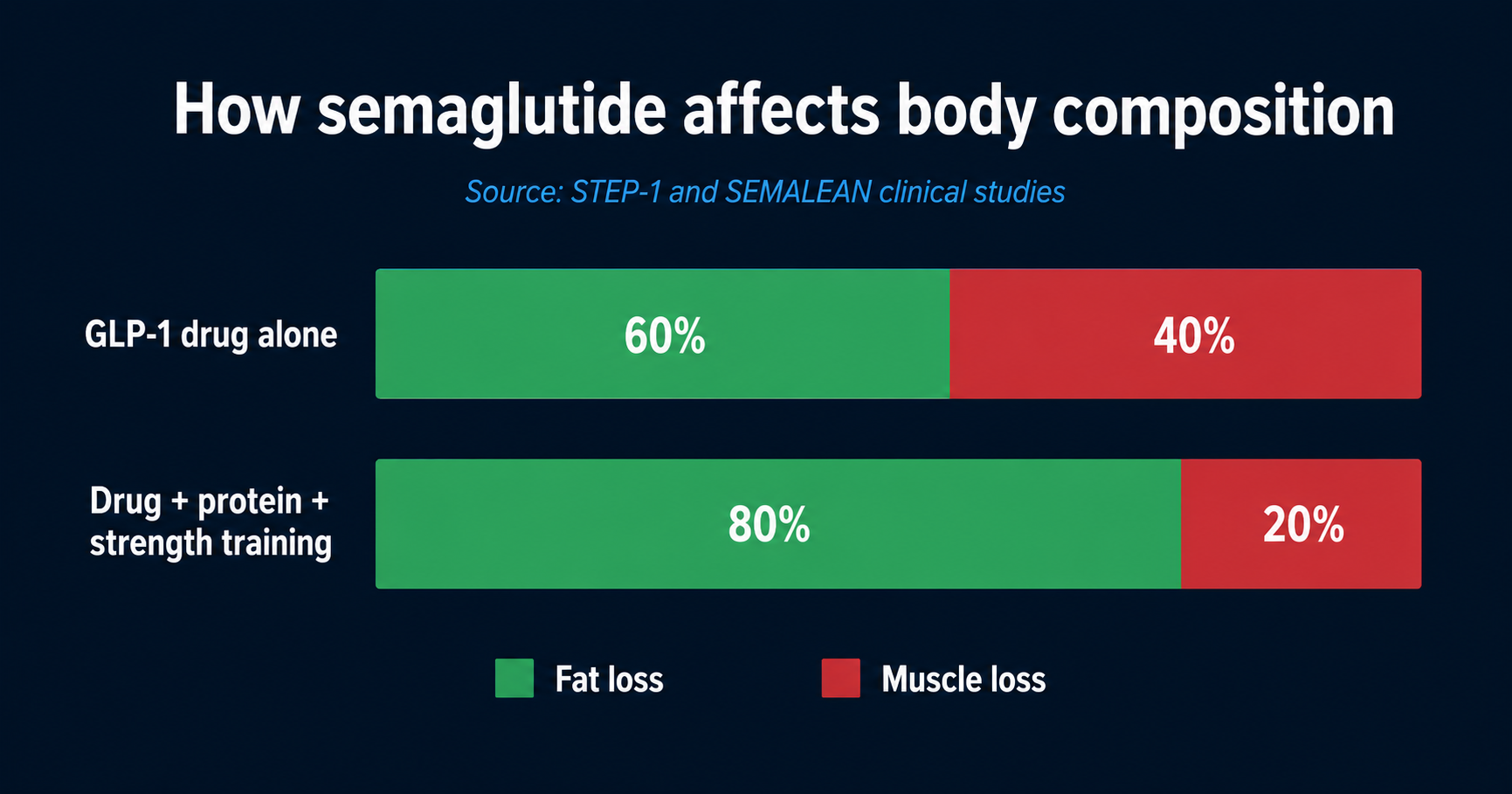
Approximately 40% of the weight you lose on semaglutide comes from lean mass — including muscle.
This isn’t a side effect. It’s the fundamental biology of rapid weight loss without resistance training and adequate protein. Your body doesn’t just burn fat; it burns muscle too.
The SEMALEAN study (2025-2026) gave us the best data on this. Patients on semaglutide 2.4 mg lost significant fat mass (14% at 7 months, 18% at 12 months), but lean mass also dropped by 3 kg in the first 7 months. The encouraging finding: lean mass stabilised after that, and handgrip strength actually improved by 4.5 kg at 12 months.
A 2025 study presented at the Endocrine Society’s annual meeting found that higher protein intake significantly reduced muscle loss in patients on semaglutide. Women and older adults were at highest risk.
What does this mean practically?
If you take semaglutide without proper nutrition and strength training, you’ll lose weight — but you’ll also lose the muscle that keeps your metabolism running, protects your joints, and determines your quality of life as you age.
This is exactly why I tell clients: the drug is not a replacement for coaching. It’s a tool that works best when paired with structured nutrition (especially adequate protein — 1.2-1.6 g/kg bodyweight) and progressive resistance training.
The Other Peptides: What Your Gym Bro Won’t Tell You
Now let’s talk about the category that genuinely worries me.
BPC-157. TB-500. Ipamorelin. CJC-1295. Growth hormone releasing peptides. These are everywhere on fitness Instagram and YouTube — promoted with dramatic before-and-after photos, affiliate codes, and zero disclaimers.
Here’s what you need to know:
- Almost no human clinical data. Most peptide research was done on rats. Some peptides were studied in humans but abandoned for failing to show benefits or for having serious side effects. The fact that something “showed promise in animal studies” means very little for human safety.
- Not regulated. These are sold as “research chemicals” — a legal loophole that lets companies sell substances that aren’t approved for human use. Quality control is minimal. You have no guarantee that what’s on the label is what’s in the vial.
- Real side effects. Reported adverse effects include nausea, vomiting, abdominal pain, immune reactions, allergic responses, infections from contaminated products, water retention, acne, and hormonal disruption.
- Influencer incentives. Many fitness influencers promoting peptides are affiliated with the retailers selling them. They get paid when you buy. They don’t get paid when you get side effects.
A May 2026 investigation published by The Conversation found that social media influencers are openly marketing these unproven injectables to average gym-goers — people who have no way to evaluate the claims being made.
This isn’t health optimisation. It’s gambling with your endocrine system based on a stranger’s Instagram story.
The THINQ.FIT Position: Informed, Not Ideological
I’m not anti-peptide. I’m anti-uninformed.
Here’s my honest breakdown:
When GLP-1 drugs (semaglutide/tirzepatide) may make sense:
- You have a BMI above 30 (or above 27 with metabolic conditions like diabetes, hypertension, or sleep apnea)
- A qualified endocrinologist or obesity medicine specialist prescribes it
- You combine it with proper nutrition (high protein, structured meals) and resistance training
- You understand it’s a long-term commitment — most people regain weight after stopping unless lifestyle changes are in place
- You get regular bloodwork to monitor kidney function, pancreatic enzymes, and thyroid
When peptides don’t make sense:
- You want to lose 5-10 kgs and haven’t tried structured nutrition first — that’s using a sledgehammer for a nail
- You’re buying BPC-157 or growth hormone peptides from an Instagram ad — you’re injecting an unregulated substance with no safety data
- You think the injection replaces eating well and training — it doesn’t, and the muscle loss data proves it
- Your friend lost weight on it and you want the same — individual responses vary dramatically, and “my friend did it” is not a medical justification
What I Actually Recommend
Before you spend ₹1,290/month (or more) on semaglutide, try this for 12 weeks:
- Get your protein right. Most Indian professionals eat 40-50g of protein per day. You need 80-100g minimum. Add paneer, curd, eggs, dal, and chicken/fish at every meal. This alone prevents muscle loss and improves satiety — the same mechanism semaglutide targets.
- Fix your meal timing. 70% of your food before 3 PM. Lighter dinners. This is what we’ve seen work across 4,000+ clients — without any drugs.
- Strength train 3x/week. 30-45 minutes. This protects muscle mass whether or not you ever take GLP-1 drugs. It’s non-negotiable for long-term health.
- Get bloodwork done. Fasting insulin, HbA1c, lipid panel, liver function, thyroid panel. Know your metabolic baseline before you make any decisions about pharmaceuticals.
If after 12 weeks of structured nutrition and training you’re still not seeing results, then — with your doctor — GLP-1 drugs become a reasonable conversation. And if you do go that route, having the nutrition and training foundation already in place means you’ll lose more fat, preserve more muscle, and be far more likely to keep the weight off.
The Bottom Line
Peptides are not magic. They’re not evil. They’re pharmaceuticals with real effects, real side effects, and real limitations.
The semaglutide revolution in India is genuinely significant — affordable generics mean more people with obesity and metabolic disease can access a tool that works. That’s a good thing.
But a tool without a plan is just a shortcut. And shortcuts, in health, have a way of becoming detours.
Get your nutrition right. Get your training right. Get your bloodwork done. Then decide.
Studies referenced: SEMALEAN study (2025-2026) • STEP-1 trial (2021) NEJM • Endocrine Society ENDO 2025 • The Conversation (May 2026) • Novo Nordisk India patent expiry (March 2026)

